Exam Checklist
- observes proper patient draping
- observes the rate, rhythm, depth, effort of breathing
- observes overall respiratory status including cyanosis and clubbing
- inspects trachea and evaluates for deviation
- inspects posterior chest
- evaluates posterior chest excursion (in at least 1 level)
- evaluates for tactile fremitus (in at least 3 levels)
- percusses the posterior and lateral chest (in at least 3 levels)
- auscultates posterior and lateral chest (in at least 3 levels)
- inspects anterior chest
- auscultates anterior chest (in at least 2 levels)
Write-up Examples
Thorax is symmetric with good expansion. Lungs resonant. Breath sounds vesicular; no rales, wheezes, or rhonchi. Diaphragms descend 4 cm bilaterally.
Thorax symmetric with moderate kyphosis and increased anteroposterior (AP) diameter, decreased expansion. Lungs are hyperresonant. Breath sounds distant with delayed expiratory phase and scattered expiratory wheezes. Fremiti decreased; no bronchophony, egophany, or whispered pectoriloquy. Diaphragms descend 2 cm bilaterally.
Notes
Evaluation for tactile fremitus, percussion and auscultation should be preferentially performed side to side and at a minimum of 3 levels on each side posteriorly.
Be aware of surface anatomy so an abnormality can be localized.
Although not part of the “pulmonary system examination” this is a good time to check for spinal tenderness and CVA tenderness.
Note that initially you may use sentences to describe the findings; later you will use phrases appropriate for most write-ups.
Remember to only use approved medical abbreviations.
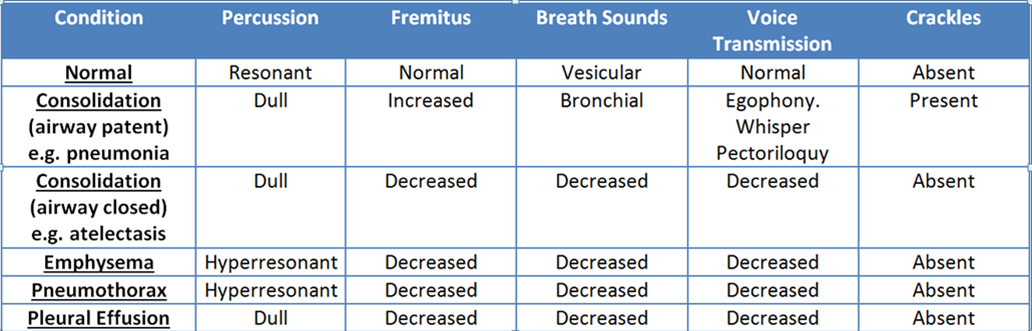
Physical Examination Findings - SIM